Obstruted Defaecation Web
| Internal Rectal Intussusception [Internal Rectal Prolapse |
|
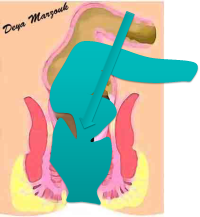
Internal Rectal Intussusception is a term that denotes that lower part of the bowel [the lower sigmoid or upper rectum] slides inside the rectum so that there will be a tube inside a tube, as seen in the Flash animation below.
What is the significance of rectal intussusception ? This is not always clear. Some asymptomatic normal volunteers undergoing defaecation proctography were found to have rectorectal Intussusception, a fact also mirrored by some asymptomatic patiebnts undergoing digital rectal examination. On the other hand some patients with recto-rectal intussusception are symptomatic, which may occur for a variety of reasons, including narrow diameter of intussuscpted bowel or associated presence of S shaped rectum, redundant sigmoid, slow colonic motility or fixed pelvic bends. Recto-anal intussusception, on the other hand is not uncommonly associated with obstructed defaecatory symptoms, even when isolated [although it can be equally associated with the factors mentioned in the preceeding paragraph]. l Which is more important, an intussusception or a rectocoele? In many patients there is an associated rectocoele as well. It is somewhat difficult to tell which is more symptomatic. I have repaired large rectocoeles for many years believing there were more significant.However in the last ten years, I came to the conclusion that intussusception was more likely to be the dominant [but not necessarily the only] cause of symptoms. Defaecation proctography may suggest that intussusception may descend low enough to impede further defaecation or may suggest that a large functional rectocoele may actually contribute more to the difficulties with evacuation. Careful patient history and examination likewise may shed light on whether both intussusception and rectocoele contribute to the difficulty with evacuation or whether one is more important. At the end the experienced coloproctologist has to make an informed judgment on what is more important and thus recommend a particular course of treatment Clinical features & Diagnosis of rectal intussusception Patients with rectorectal intussusception may be asymptomatic, although more commonly will cope with mild obstructed defaecation symptoms. This will include symptoms such as mild change in bowel habits, with characteristic "interrupted defaecation" in the morning Patients with rectoanal intussusception have more severe obstructed defaecation symptoms including severe straining, incomplete evacuation and sometimes complete failure to defaecate from time to time. Some patients may report the need to use fingers to "fish" faecal pellets from the rectum or support the perineum during defaecation. Many will complain of urgency, frequency or even episodes of incontinence. The diagnosis is easy for the experienced pelvic floor clinician. These can be enhanced by the 2 clinical tests I developed [the hook & the corckscrew tests, see in video section]. straining while the patient is examined with proctoscope differentiate between type 2 [recto-anal intussusception] & type 3 [internal-external intussusception]. Clinical diagnosis is confirmed by proctography. If proctography fails to demonstrate intussusception [especially in patients who do not defaecate the test stool fully], then it is more than likely that the clinical impression [on DRE] is more accurate Treatment options These are discussed more in other web pages on this site, but briefly there is a great deal of controversy about best management, largely due to the fact that this condition is poorly understood by most colorectal surgeons & gastroenterologists All patients [with the exception of those with severe symptoms AND internal-external intussusception] should be offered conservative treatment first [patient education, avoid straining, suppositories etc.]. If this fails then patients should be offered trans-anal rectal irrigation. I no longer believe that biofeedback is useful in the initial management of these patients, but it may still play a role in postoperative management. If conservative treatment fails then patients should be offered surgery.Surgical treatment of obstructive defaecation is still controversial. The number of studies evaluating different approaches is small and the number of patients treated in each series is also small. Pioneering surgeons in the field hold strong views on one approach or another, without strong evidence in most cases. Patients need to be made aware of the different options and should be involved fully in the discussion prior to surgery, emphasizing that these procedures may improve, but not necessarily cure obstructive defaecatory symptoms altogether. It is also very important to emphasize what is being treated here, which is an anatomical abnormality that appear to interfere with the mechanics of defaecation. Surgery can not be expected to change disordered sensation and thus may not help certain syptoms. 1. Laparoscopic deep pelvic dissection [down to anal canal], rectopexy & anterior resection. This operation not infrequently is combined with cul-de-plasty, colposacropexy and or uterine suspension. This is [in my view] by far the best option and is my current preferred treatment option. Almost all patients can be done laparoscopically. This has the distinct advantage of dealing with all the factors contributing to the patient's ODS. Not only one can deal with all rectal wall abnormalities (the internal rectal intussusception, S shaped rectum fixed to the pelvic side wall and any rectocoeles), but will also deal with sigmoid causes of ODS (long redundant sigmoid, sigmoidocoeles, sigmoid stuck to vagina following hystrectomy or severe diverticular disease) and can treat enterococeles simultaneously by lifting the pouch of Douglas upwards and adding a cul-de-plasty. Furthermore, there is an opportunity to hitch the uterus up [uterine suspension] in patients in whom abnormal uterine descent blcok rectal lumen on straining & finally it affords a chance to treat vaginal vault prolapse by incorporating colposacropexy. In my view the options below [2-5] are far less successful, because they would deal only with the intussusception & not always very effectively. Adding laparoscopy to these operations can improve outcome by selecting those patients whose symptoms can be attributed to internal intussusception or rectocoele only. It also affords a way to air test rhe integrity of any anastomosis performed. These procedures are discussed further under Treatment options: Surgery 2. Laparoscopy & Trans-Starr 3. Laparoscopy & traction Tran-Starr [traction REPLACE] 4. Intra-anal Delorme's Procedure 5. Express procedure (Norman Williams) |